Now and Then
By Iris Winston
My friend did not enjoy the organ recitals that were a regular part of social interactions in his twilight years. He didn’t mean musical serenades. Instead, he was talking about the way many of his acquaintances regaled him with details of the dysfunction of their various organs as they aged.
Now that I am in the organ-recital years, I make a conscious effort not to talk about any issues I have with assorted body parts. However, when people make a polite query about my health, I do qualify my answer.
 “I’m fine, except for my knees.”
“I’m fine, except for my knees.”
That periodically leads to a short discussion about the cause of the problem—severe osteoarthritis in my case—and sometimes comparison with similar symptoms in the person who asked how I was (and probably now regretted the question).
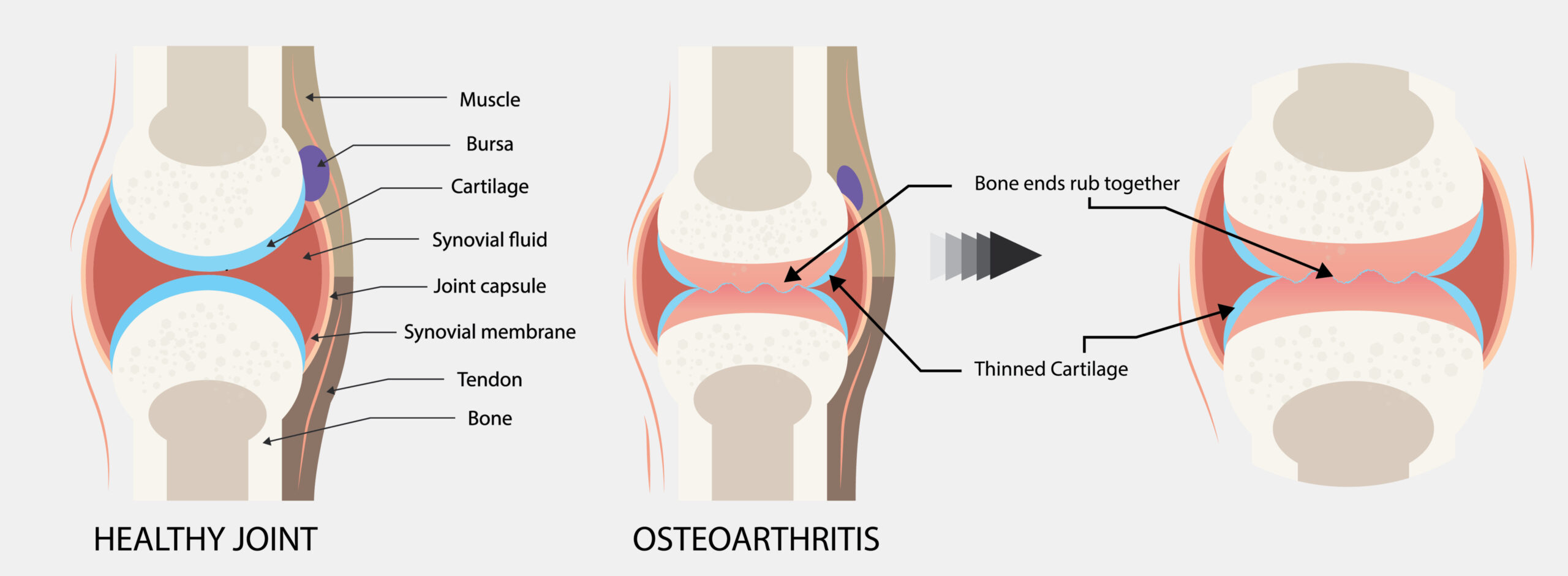
Osteoarthritis, a progressive, degenerative disease of the joints, leads to the breakdown of cartilage and the underlying bone. Sometimes described as a “wear and tear” disease, osteoarthritis can damage any joint, but most often affects hands, knees, hips and spine. Among the symptoms are swelling and deformity of affected joints, as well as pain and stiffness, particularly after a period of inactivity.
A common disease that affects millions of people globally, the primary risk factor is age. Think of how many older folk comment on their aches and pains, especially in damp weather. Another risk factor is gender. More women than men develop osteoarthritis. Genetics also plays its part. If a parent suffered from osteoarthritis, you are also likely to develop it. Other factors such as sport or work-related injuries, accidents and repetitive activities increase the chance of developing the disease, as do being overweight, eating unhealthy foods and leading a sedentary lifestyle. The old mantra of “use it or lose it” definitely applies with arthritis.
This is why managing an incurable disease is front and centre. A healthy diet that contains plenty of fruits and vegetables, followed by regular exercise, is a good starting point. My dog and I go for two walks a day. (More accurately, it’s one walk and one visit to the dog park, where he runs and I don’t walk far, though my legs are in weight-bearing mode.)
Some oral and topical medications, as recommended by my family doctor, also help to reduce inflammation and pain. The cortisone injections she administers every few months bring further relief for a time.
Last year, after being checked at the assessment clinic in the Queensway Carleton Hospital, I was referred to the GLA:D program at the Almonte General Hospital. GLA:D (Good Life with osteoArthritis in Denmark) is a series of graduated exercises that originated in Denmark to help people with arthritis cope with symptoms under supervision and instruction from a physiotherapist. The exercise routine continues at home after the six-week course is finished. I was pleased to find how much the course—while exhausting and sometimes very challenging — has helped me. Home-based exercises are now in progress at the gradually increasing levels the physiotherapist recommended.
 My goal is to avoid knee surgery while remaining mobile. The detailed explanation the physiotherapist at the assessment clinic offered increased my reluctance to have the surgery, despite being on the waiting list to see a surgeon. I knew knee surgery was more complex than hip replacement and had a lower success rate. And, as I requested, the physiotherapist called a spade a spade. She said full recovery generally takes more than a year and most people who opt for the surgery (usually people well under 80) regret it initially, though later the majority are happy with the result. For the first six to eight weeks after the procedure, the patient must not drive, walk the dog or live alone. In addition, surgery of any kind always comes with risks. I would have to go through the process twice, as both my knees are affected.
My goal is to avoid knee surgery while remaining mobile. The detailed explanation the physiotherapist at the assessment clinic offered increased my reluctance to have the surgery, despite being on the waiting list to see a surgeon. I knew knee surgery was more complex than hip replacement and had a lower success rate. And, as I requested, the physiotherapist called a spade a spade. She said full recovery generally takes more than a year and most people who opt for the surgery (usually people well under 80) regret it initially, though later the majority are happy with the result. For the first six to eight weeks after the procedure, the patient must not drive, walk the dog or live alone. In addition, surgery of any kind always comes with risks. I would have to go through the process twice, as both my knees are affected.
GLA:D seemed a better option. I am generally free of pain when my knees are not bearing weight. I still find it painful to walk carrying anything, trying to negotiate uneven ground or negotiating stairs. I also stiffen up if I forget to move around every few minutes. But I remain hopeful that continuing the graduated exercises will keep the osteoarthritis in my knees at bay for a good while.
****
I just reached the top of the waiting list to see the surgeon of my choice. The consultation was helpful. While I have not opted for surgery yet, I have complete faith in this surgeon, who will keep me on his books for two years. As well as further X-rays and a second consultation next year, he invited me to call if I had a further problem and needed help.
I have also just discovered shockwave therapy and tried a sample treatment which had an immediate effect. While approved by Health Canada, shockwave therapy is not covered by provincial health insurance. However, for present and retired federal public servants, it is subsidized if administered by a licensed physiotherapist. For now, this is my next chapter on knees.



